Attention-deficit/hyperactivity disorder (ADHD) is a neurodevelopmental condition characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with daily functioning. ADHD executive function is described as a central mechanism underlying difficulties with planning, working memory, attention control, time management, and behavioral inhibition.
Modern medicine explains ADHD as a disorder involving altered activity in the prefrontal cortex and fronto-striatal circuits, including the basal ganglia and striatum. In Korean medicine, the condition is understood as a disturbance of systemic regulation involving qi, blood, yin, and the functional stability of the mind.
Korean Medicine Neuropsychiatry integrates these explanatory frameworks by examining how neural regulation and whole-body physiological balance are associated with attention and behavioral control. The Korean Society of Oriental Neuropsychiatry studies the relationship between psychiatric symptoms, nervous system function, and Korean medicine pattern identification.
Overview
ADHD is considered to be a neurodevelopmental condition rather than a personality characteristic or a simple lack of effort. Its symptoms reflect differences in systems responsible for regulating attention, motivation, action selection, and inhibition. The concept of ADHD executive function helps explain why a person may understand what needs to be done but still experience difficulty beginning, organizing, or completing the task.
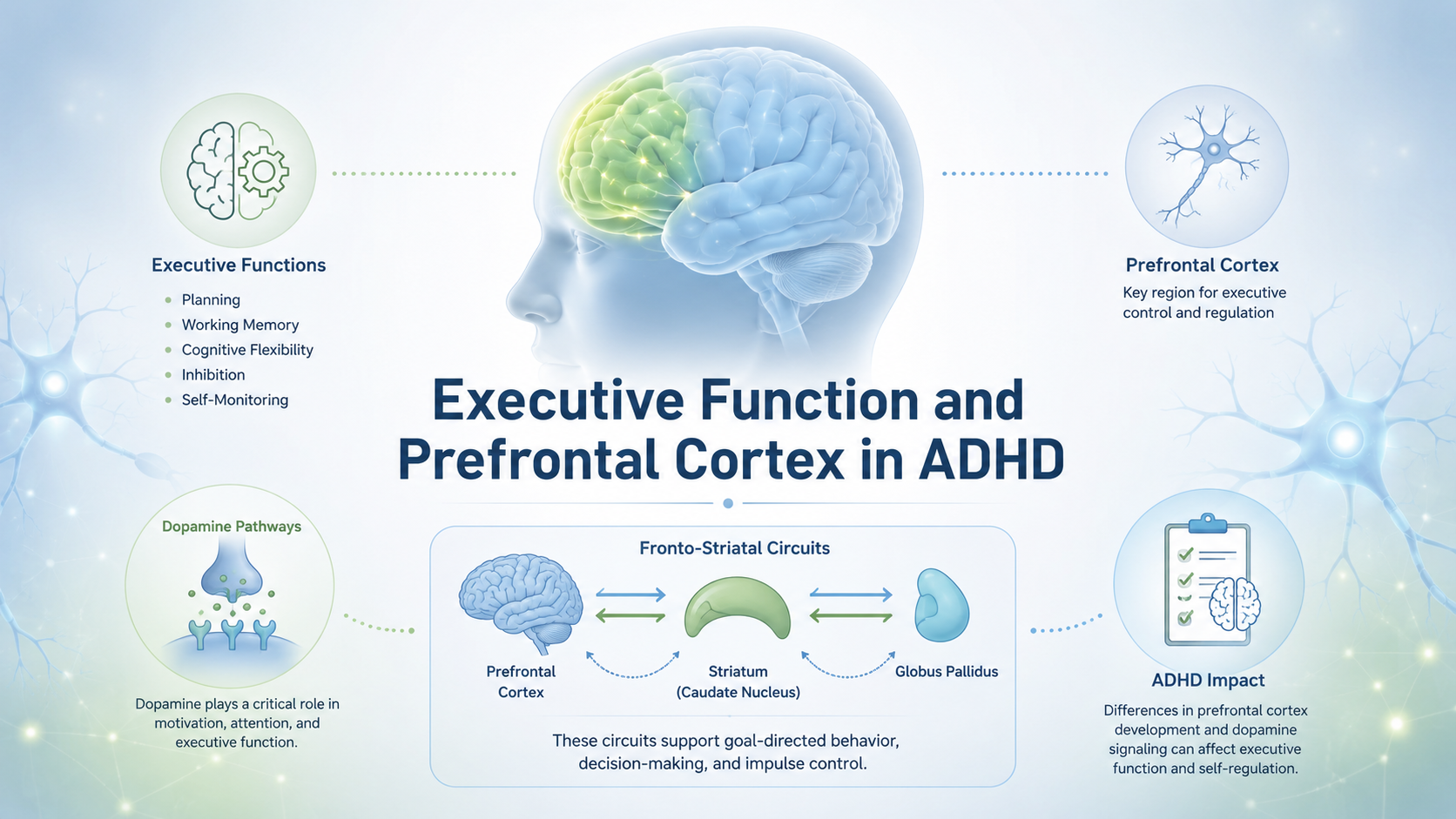
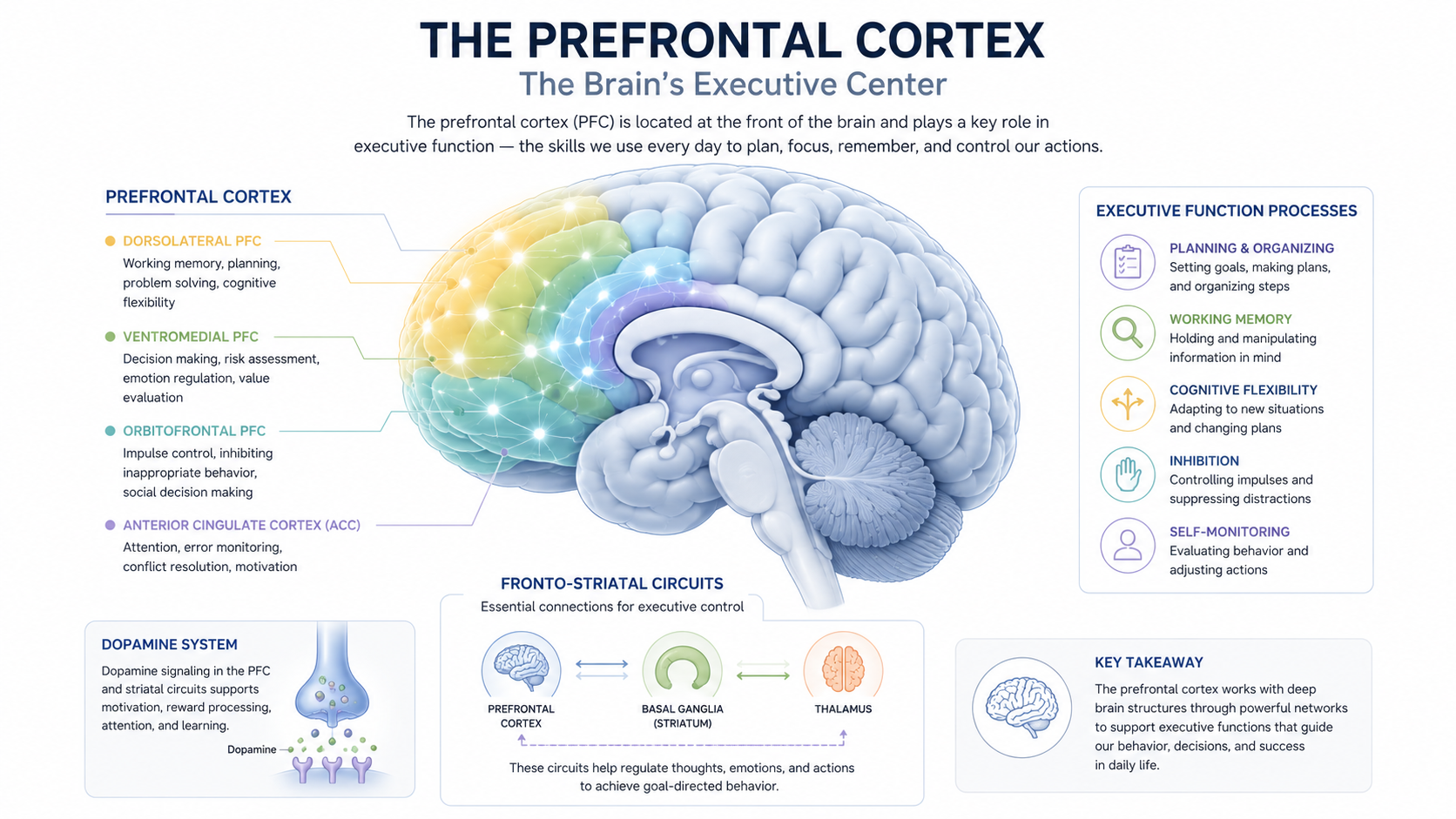
Executive function is described as a group of higher-order cognitive abilities that coordinate goal-directed behavior. These abilities include working memory, cognitive flexibility, planning, prioritization, emotional regulation, self-monitoring, and response inhibition. Executive function does not refer to a single skill or one isolated brain area. It is associated with coordinated activity across multiple neural networks.
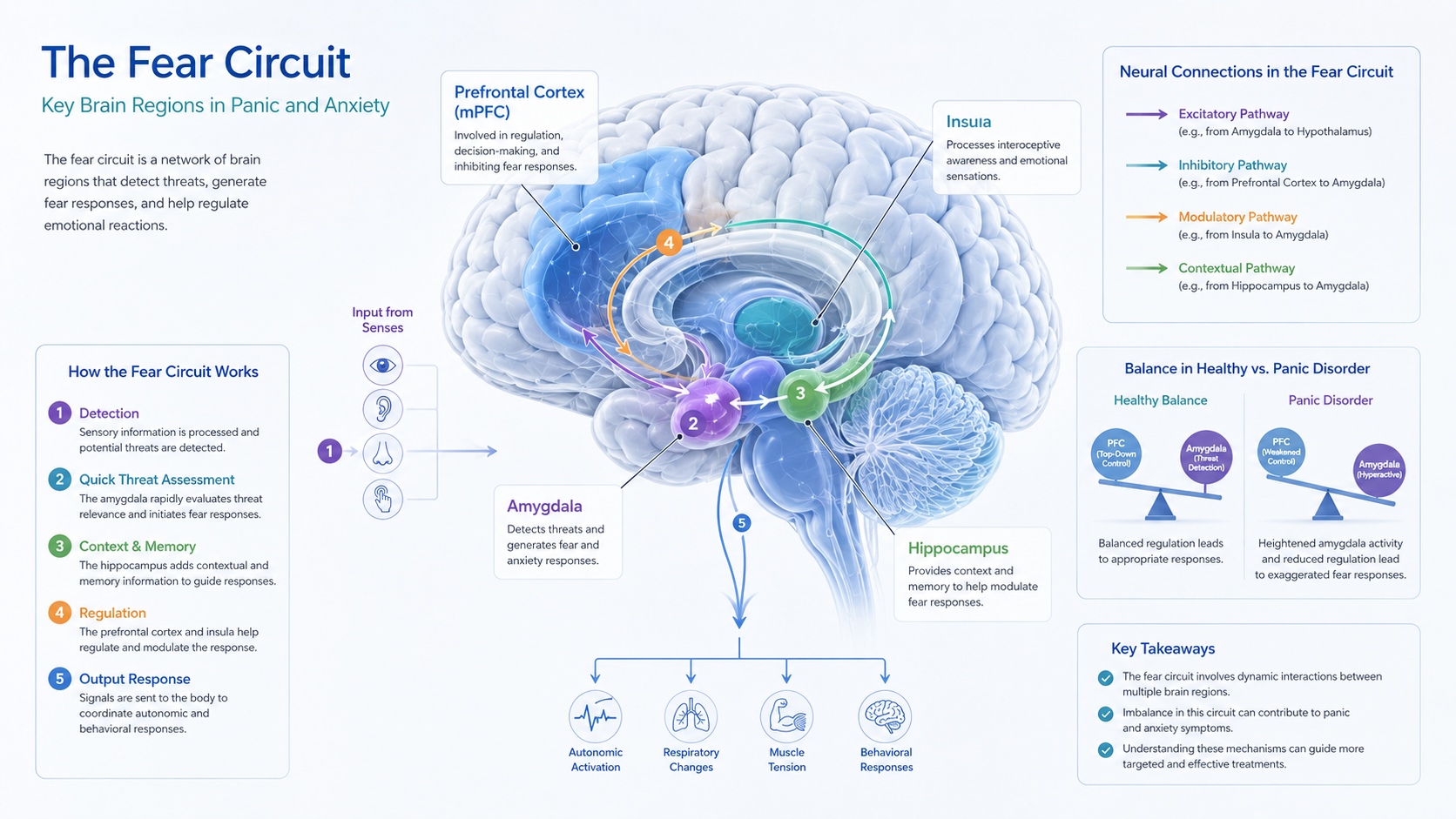
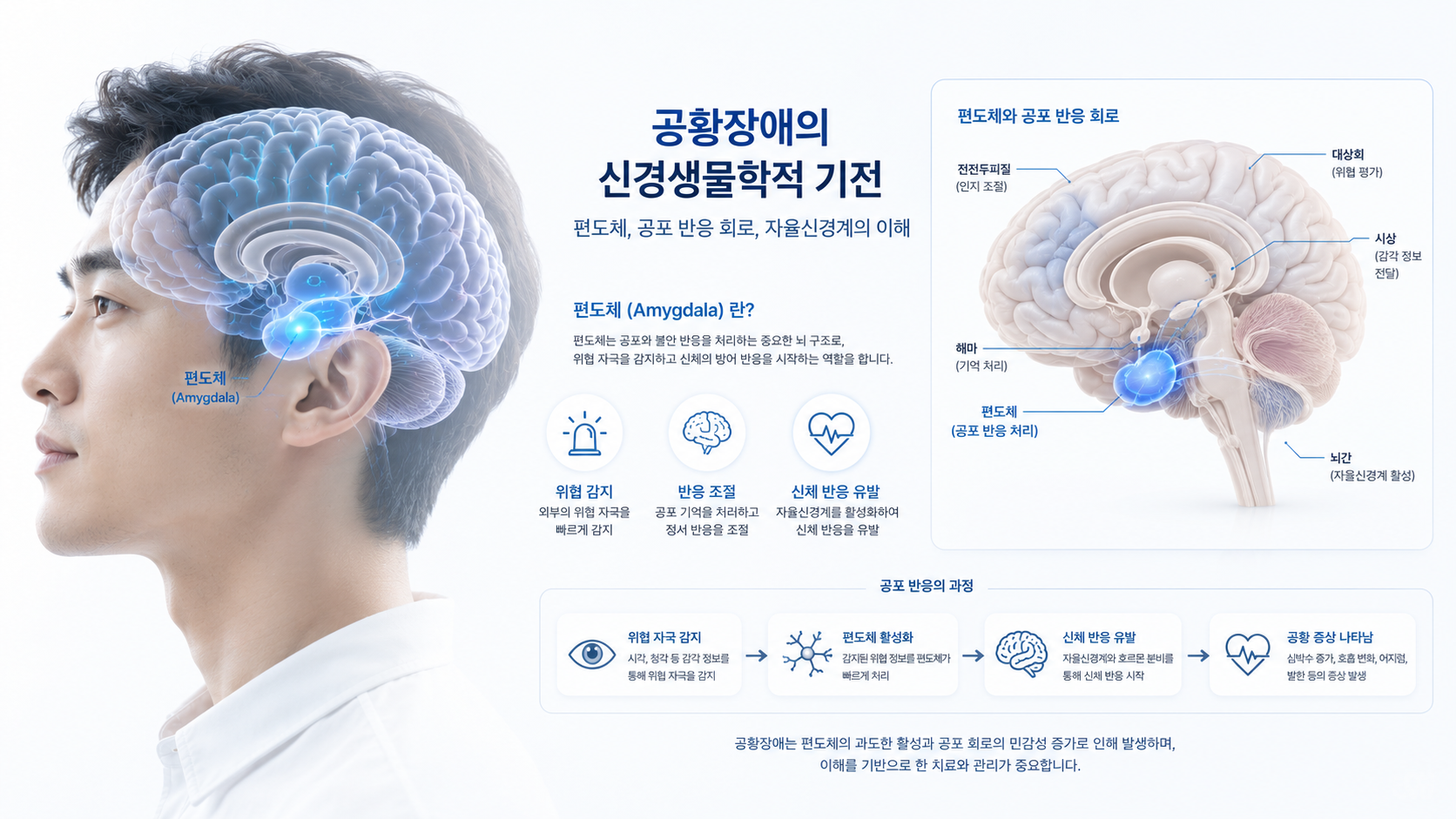
The prefrontal cortex plays a major role in maintaining task goals, evaluating consequences, suppressing unsuitable responses, and adjusting behavior according to changing circumstances. ADHD executive function impairment may be explained by reduced efficiency in the interaction between the prefrontal cortex, basal ganglia, striatum, and other regions involved in attention and motivation.
For a broader understanding of symptom patterns, see ADHD symptom overview.

Clinical Features
The core clinical features of ADHD include inattention, hyperactivity, and impulsivity. Their expression varies according to age, developmental stage, environment, and individual characteristics. Hyperactivity may appear as visible movement in childhood, while in adulthood it may be experienced as internal restlessness, impatience, or difficulty remaining mentally settled.
Inattention is described as difficulty sustaining attention, particularly during repetitive or delayed-reward activities. A person may overlook details, lose necessary items, forget appointments, or move between tasks without completing them. These patterns are associated with ADHD executive function difficulties involving working memory, task sequencing, and self-monitoring.
Impulsivity is understood as difficulty delaying a response long enough to consider its likely consequences. It may appear as interrupting, answering prematurely, making rapid decisions, or reacting strongly to immediate emotional cues. These behaviors may be explained by reduced inhibitory control and unstable regulation of reward-related signals.
Common functional effects
- Difficulty estimating how long a task will take
- Frequent postponement of tasks requiring sustained concentration
- Inconsistent performance despite adequate knowledge or ability
- Problems organizing schedules, materials, or priorities
- Emotional responses that occur faster than reflective control
- Academic, occupational, relational, or household impairment
Functional impairment is an important part of clinical evaluation. Occasional distraction alone does not establish ADHD. Symptoms are considered clinically significant when they are persistent, developmentally inappropriate, present across relevant contexts, and associated with meaningful impairment.
Etiology
ADHD has a multifactorial etiology. It is associated with genetic vulnerability, differences in brain development, neurotransmitter regulation, stress exposure, sleep, and environmental demands. No single factor adequately explains every individual presentation.
ADHD neurobiology is further described in academic research on brain function and attention regulation. National Institute of Mental Health ADHD overview provides additional scientific context.
Prefrontal Cortex and Executive Regulation
The prefrontal cortex is associated with the maintenance of goals, evaluation of competing information, inhibition of automatic responses, and adjustment of behavior. ADHD executive function impairment may be explained by reduced consistency in these regulatory processes rather than by a complete absence of executive ability.
Performance may fluctuate according to novelty, urgency, personal interest, emotional significance, and the immediacy of reward. Consequently, an individual may concentrate intensely on one activity while finding it difficult to begin another activity of equal objective importance.
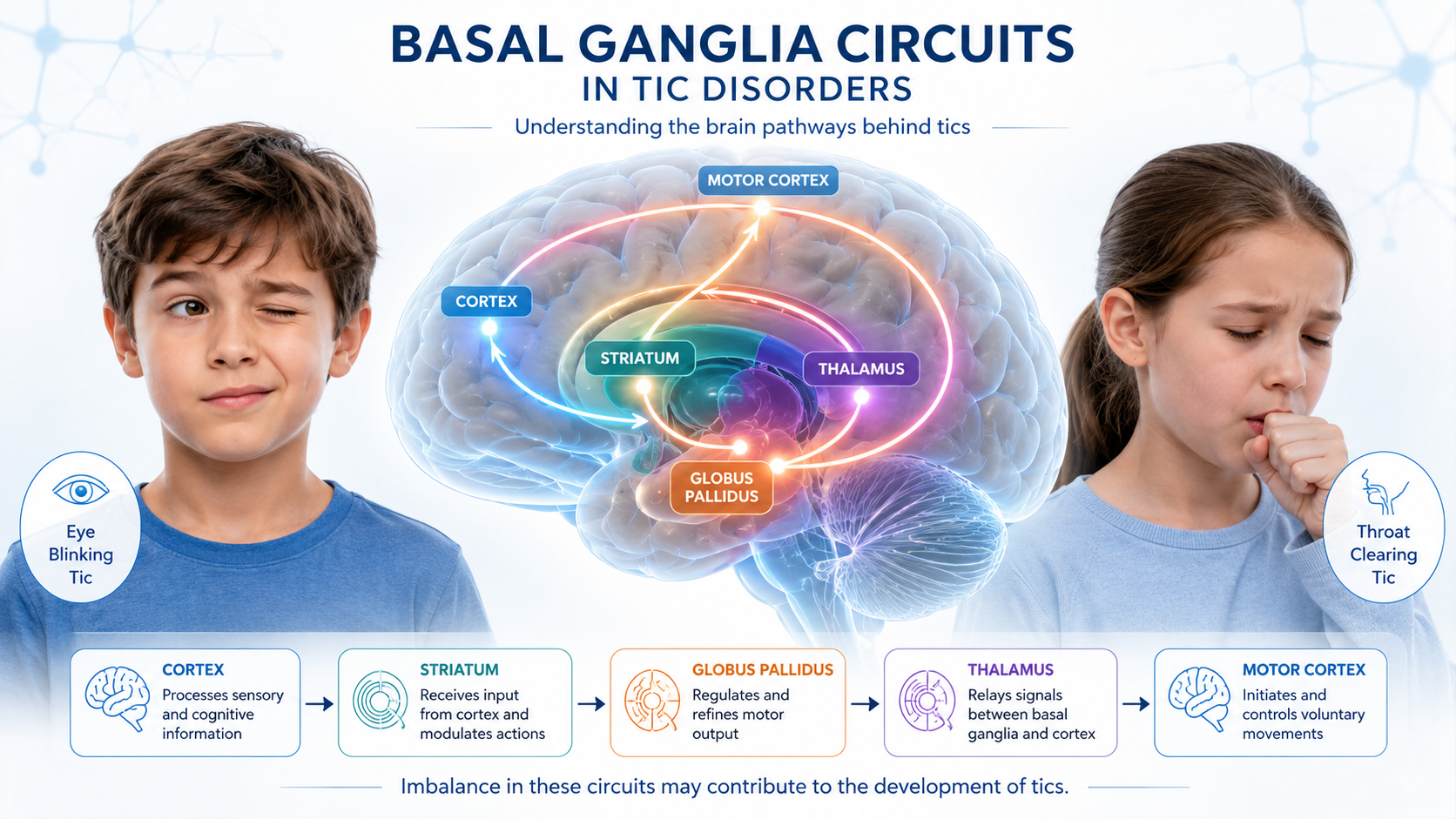
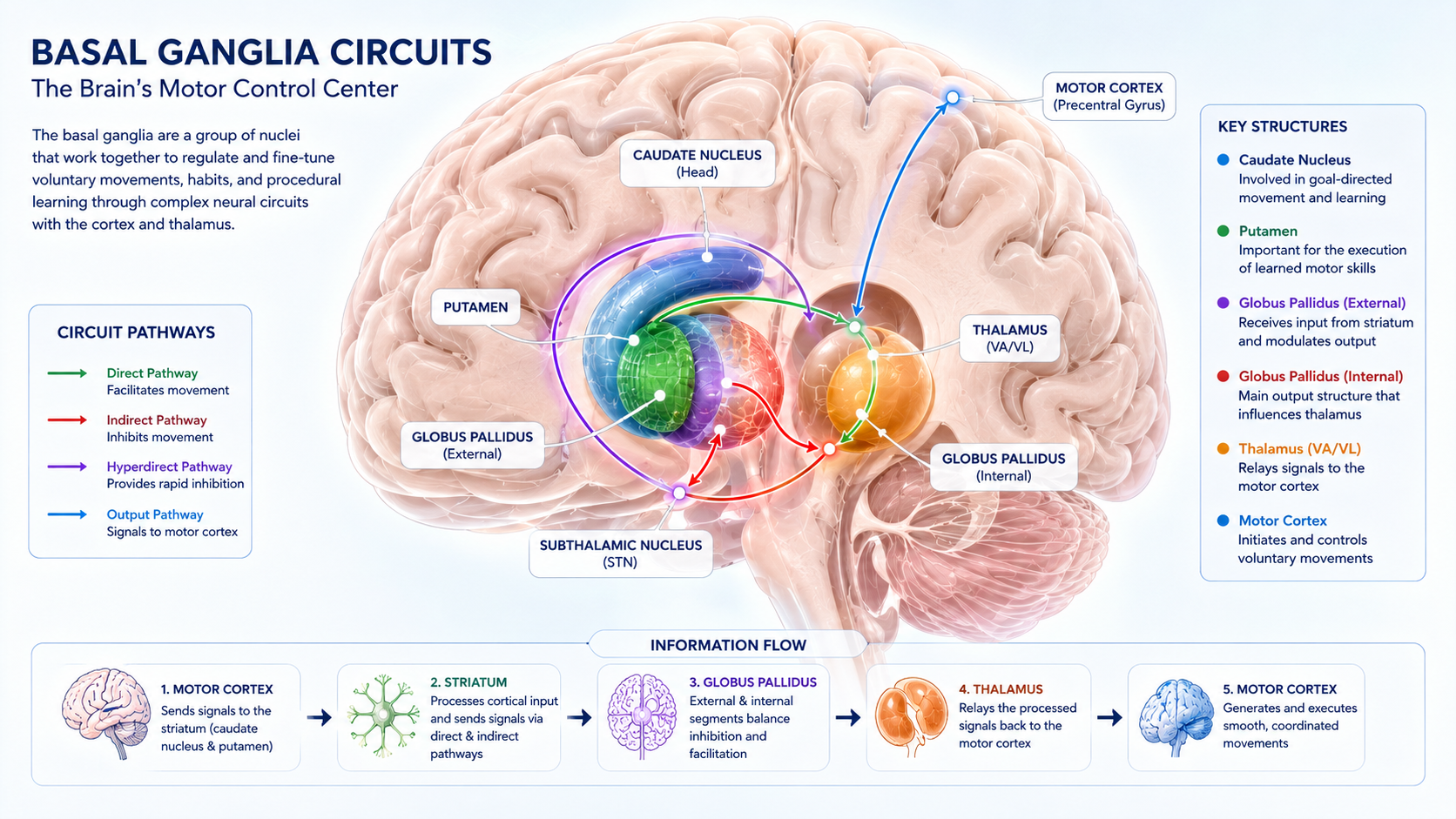
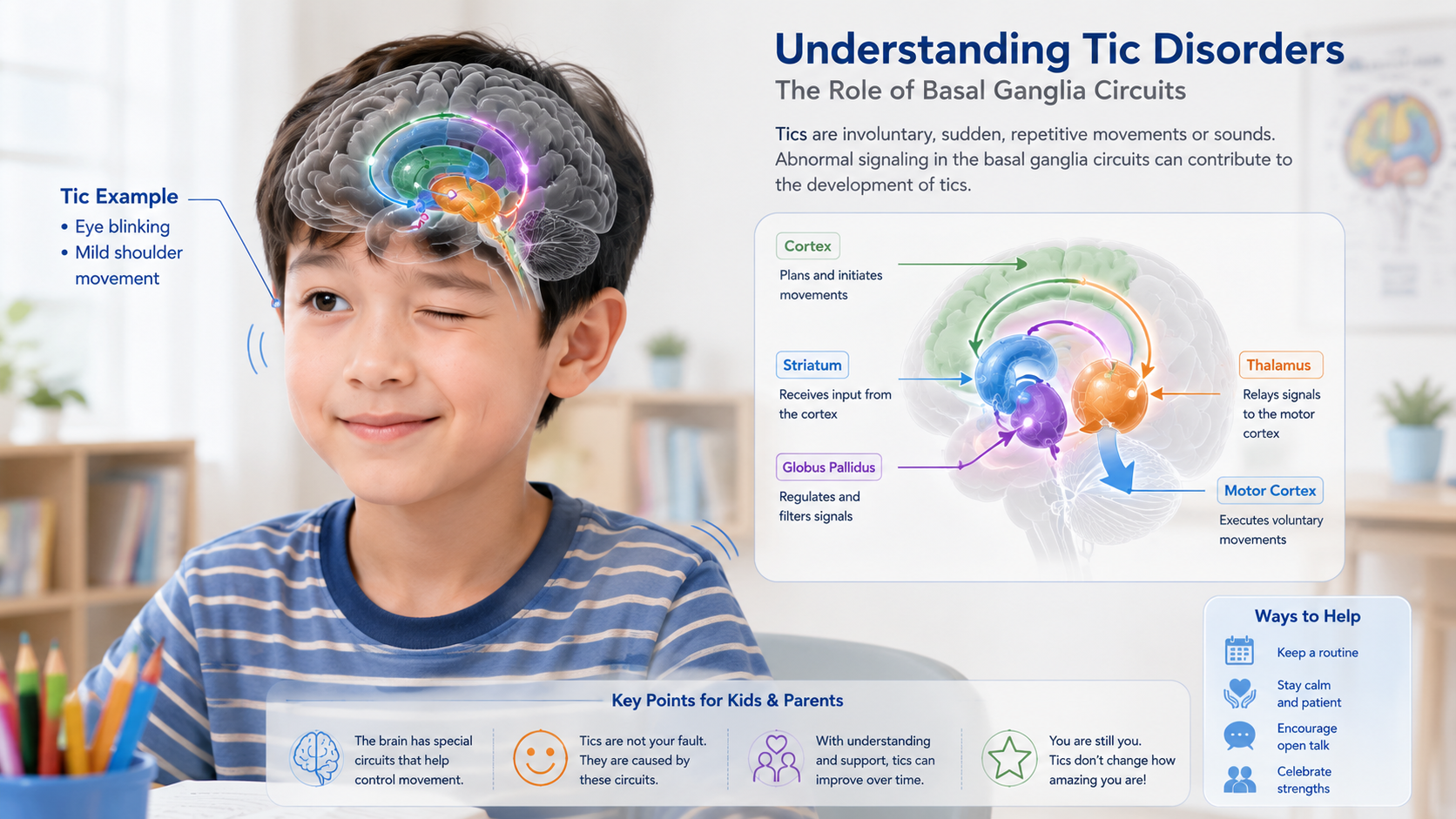
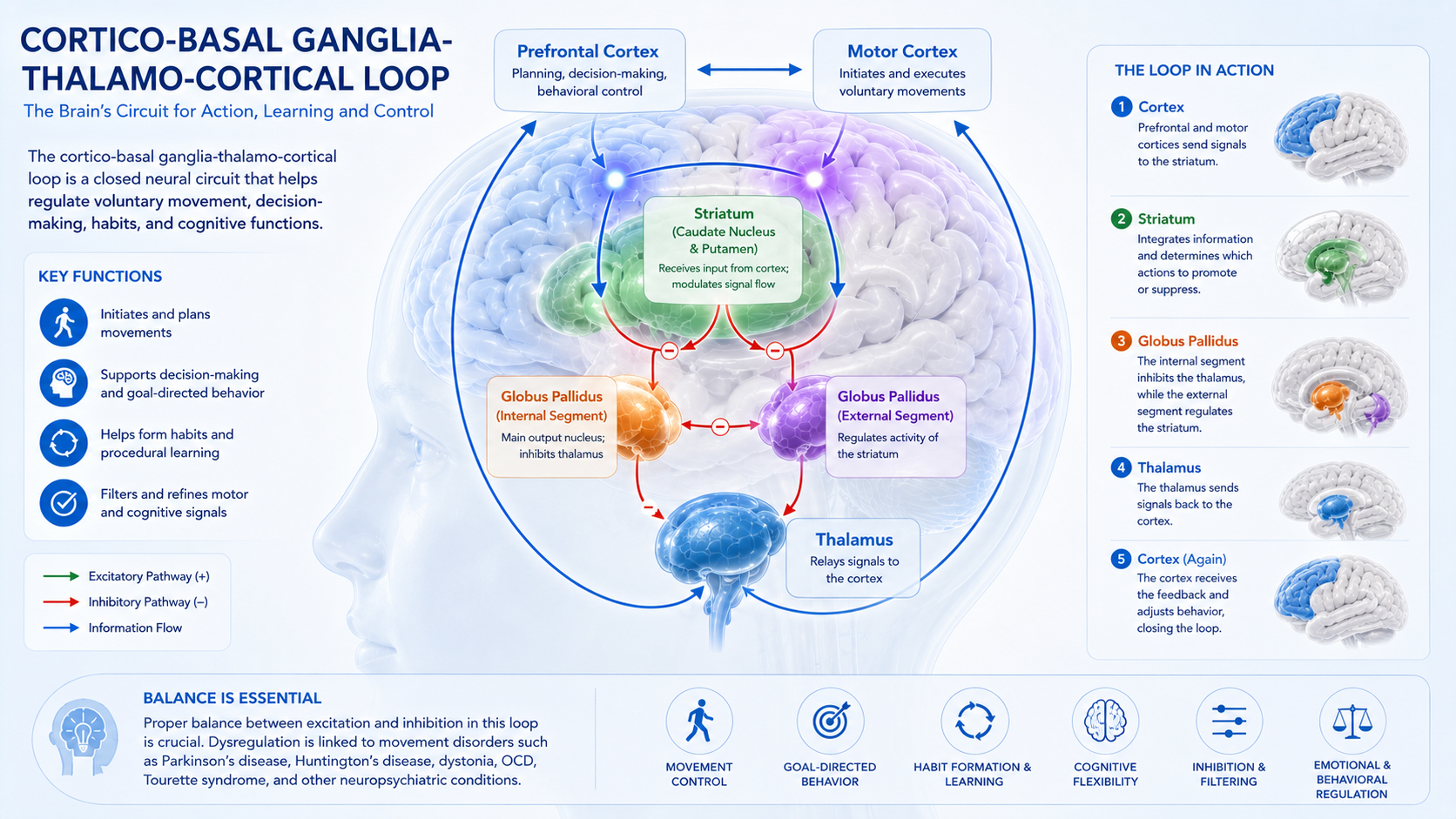
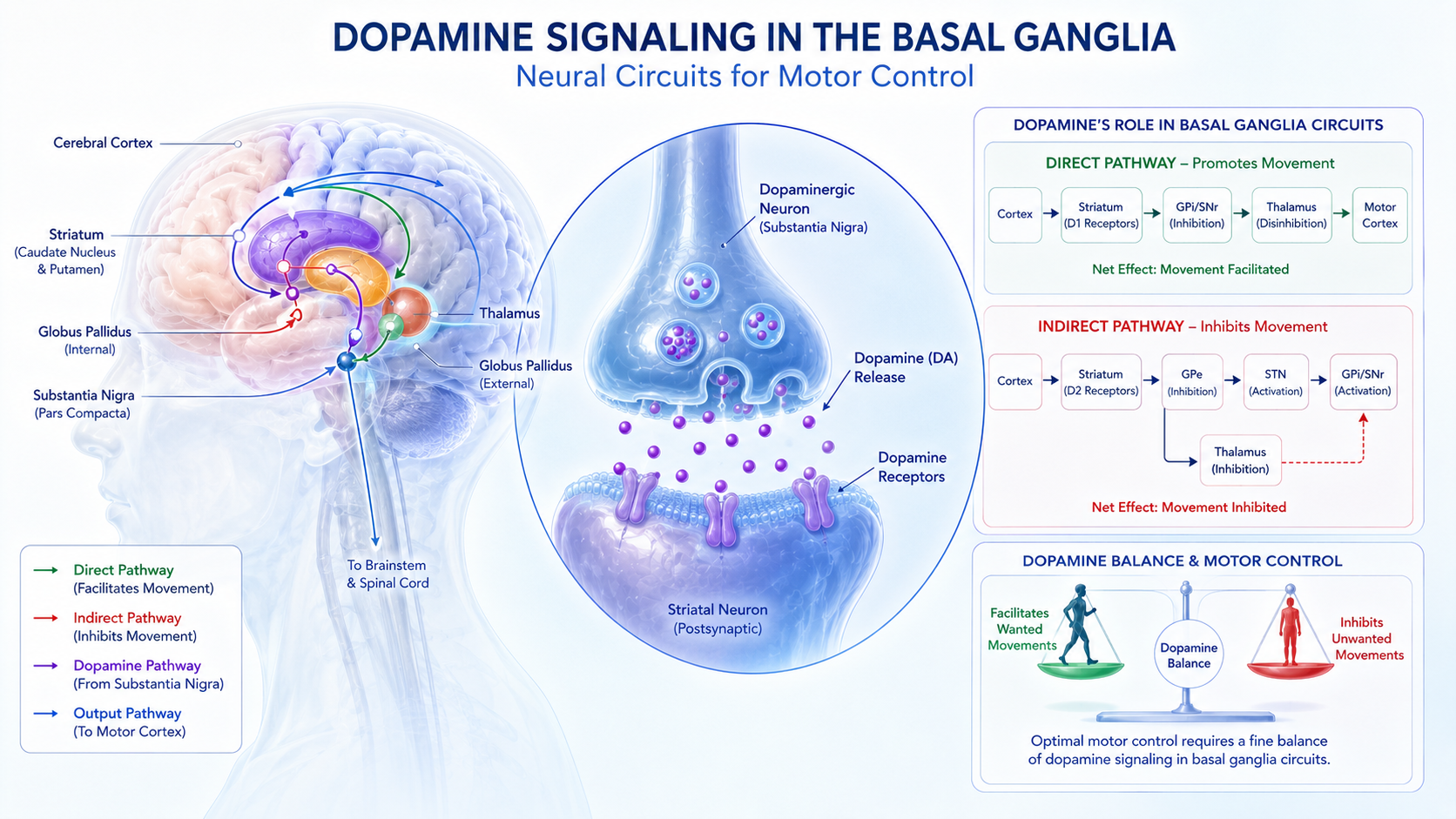
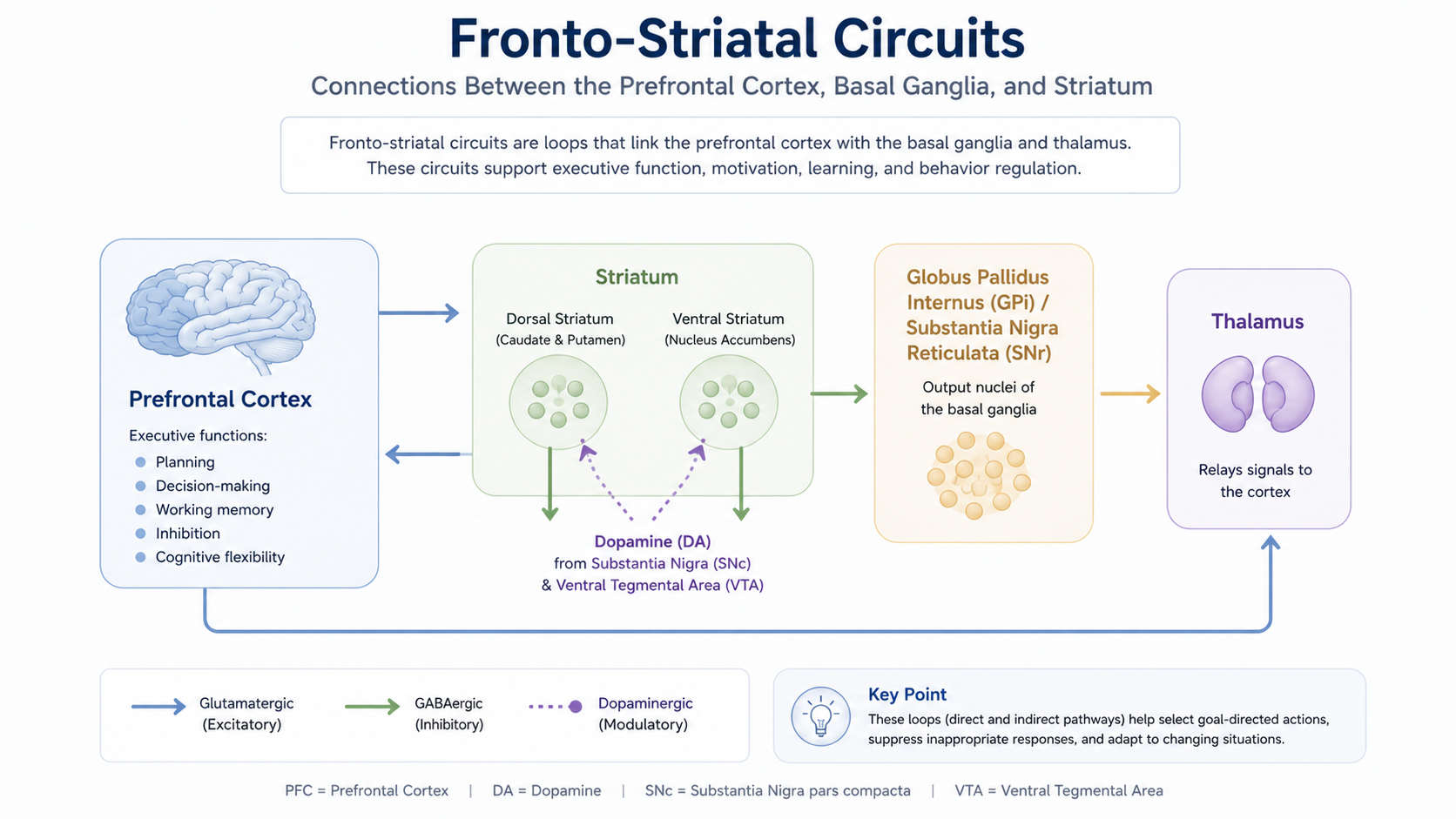
Basal Ganglia, Striatum, and Fronto-Striatal Circuits
The basal ganglia and striatum contribute to action selection, reward learning, habit formation, motor regulation, and motivational processing. Fronto-striatal circuits connect these regions with the prefrontal cortex and are considered to be central pathways in the neurobiology of ADHD.
Altered fronto-striatal communication is associated with difficulty maintaining effort when rewards are delayed. It may also contribute to impulsive choices, variable reaction time, and difficulty suppressing responses that are immediately available but not aligned with a long-term goal.
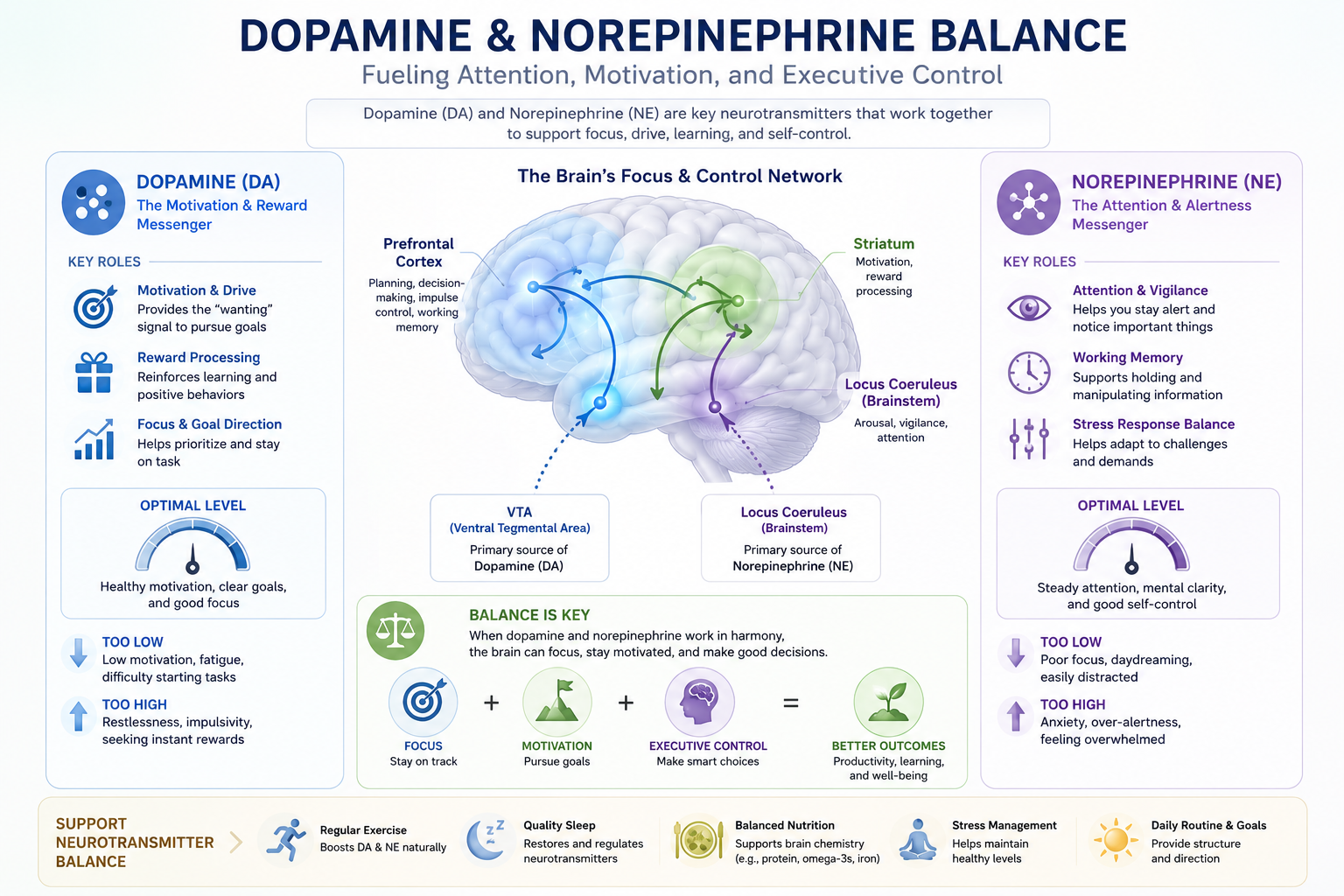
Dopamine and Norepinephrine
Dopamine and norepinephrine are important neurotransmitters in attentional regulation, motivation, working memory, and response selection. Dopamine is associated with reward prediction, reinforcement, and motivational salience. Norepinephrine is associated with alertness, signal detection, and the maintenance of task-relevant information.
Dysregulation of these neurotransmitter systems may reduce the signal-to-noise efficiency of prefrontal networks. ADHD executive function difficulties may therefore become more evident when a task requires sustained effort without immediate feedback or reward.
Stress and Environmental Influences
Environmental conditions do not provide a single explanation for ADHD, but they may influence symptom intensity and functional outcomes. Chronic stress, inconsistent routines, excessive cognitive demands, sleep disruption, and frequent interruptions can increase the burden on already vulnerable executive systems.
Supportive structure, predictable routines, task segmentation, and reduced environmental distraction may improve functional performance. Such improvement does not mean that ADHD was caused only by the environment. It indicates that executive abilities are sensitive to the interaction between neurodevelopmental characteristics and contextual demands.
Physiological System Changes
ADHD is also associated with differences in arousal and physiological regulation. Effective attention requires neither maximum arousal nor complete relaxation. It depends on an appropriate level of activation that allows the brain to distinguish relevant signals from competing information.
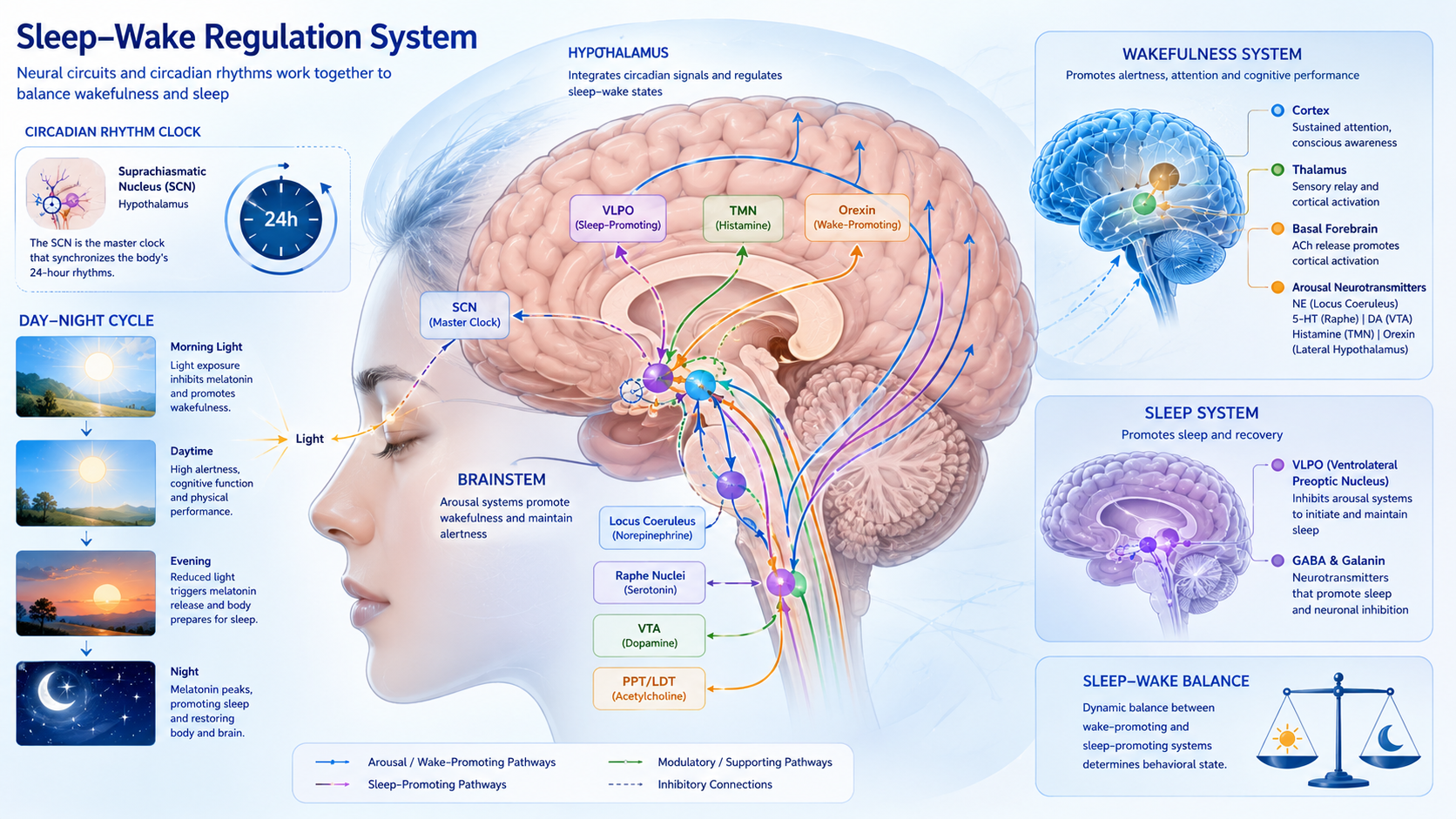
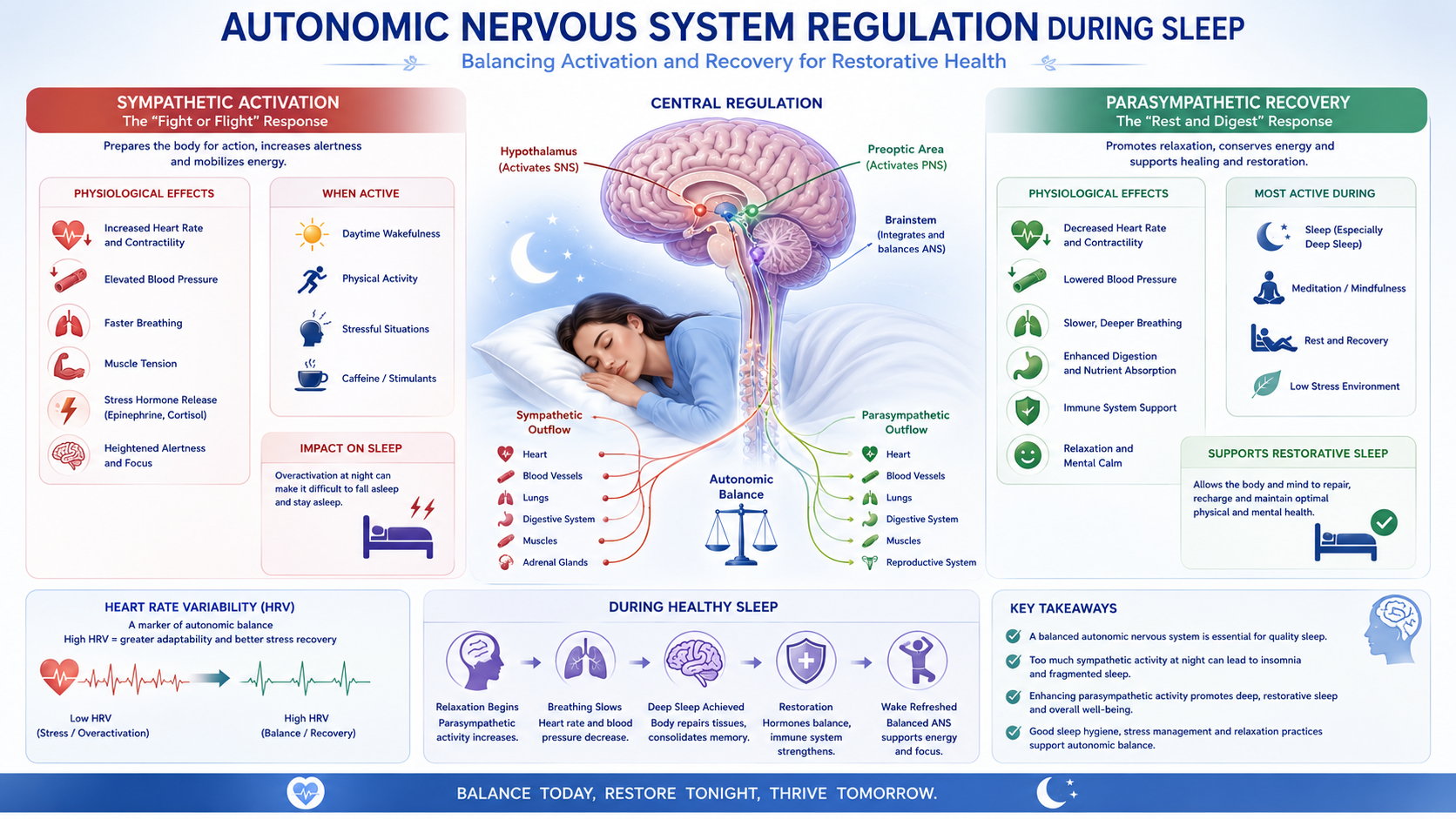
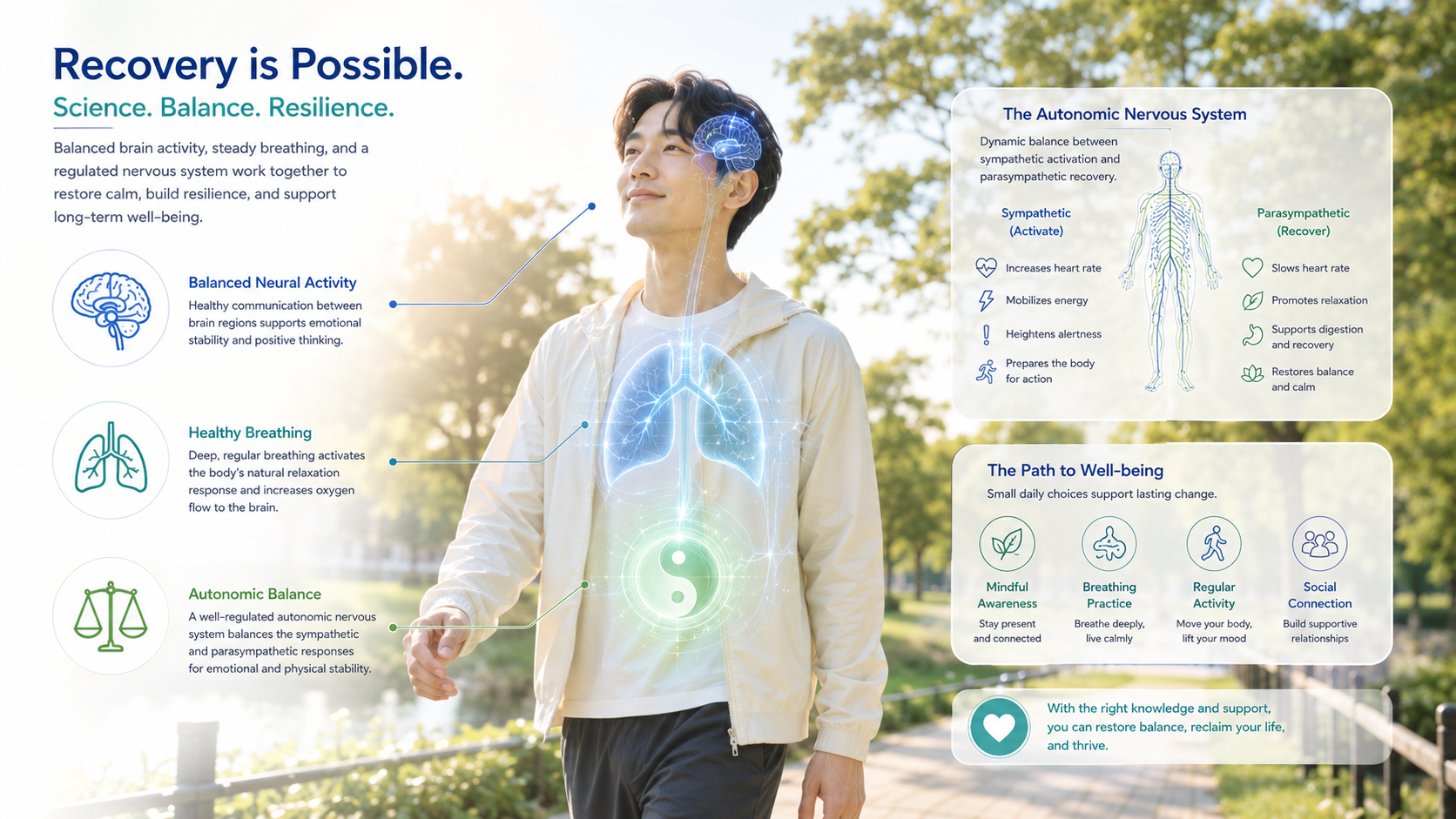
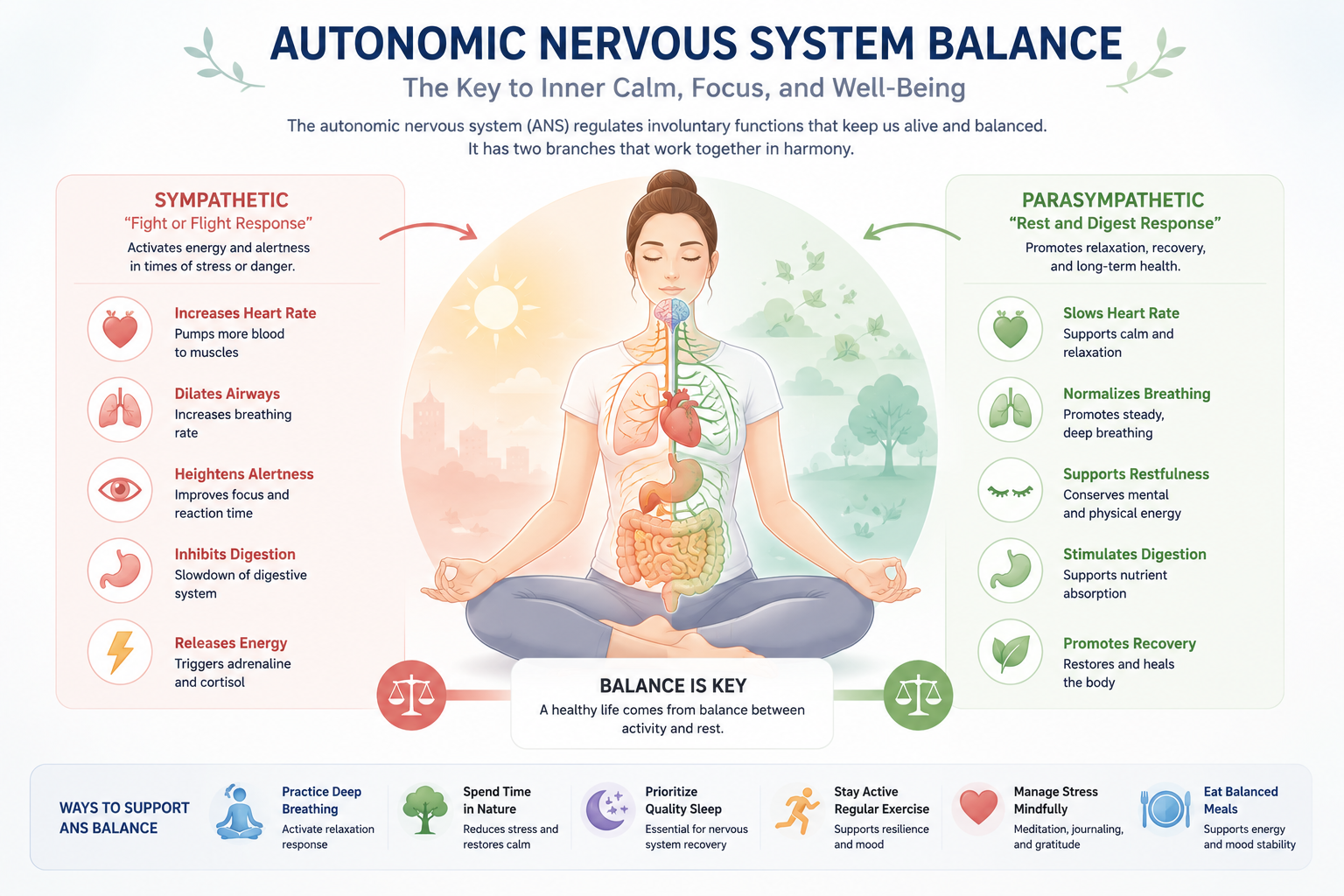
Autonomic Nervous System
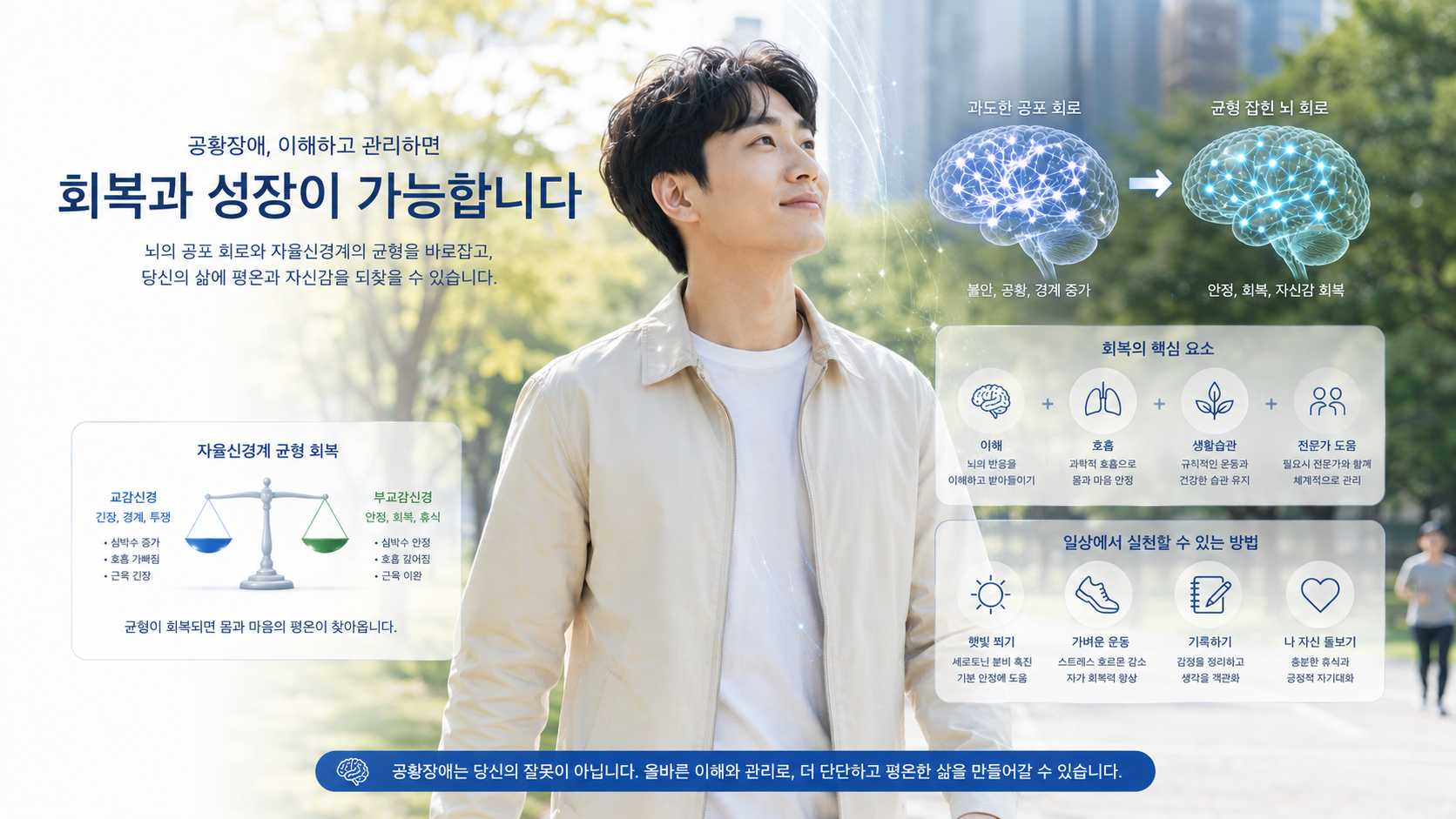
The autonomic nervous system regulates bodily functions such as heart rate, respiration, vascular tone, and physiological readiness. Its sympathetic branch supports mobilization, while its parasympathetic branch supports restoration and flexible regulation.
Some individuals with ADHD may experience unstable arousal, shifting between underactivation and excessive activation. Underactivation may be associated with low task engagement or the need for stronger stimulation. Excessive activation may be associated with restlessness, emotional reactivity, or difficulty disengaging from immediate stimuli.
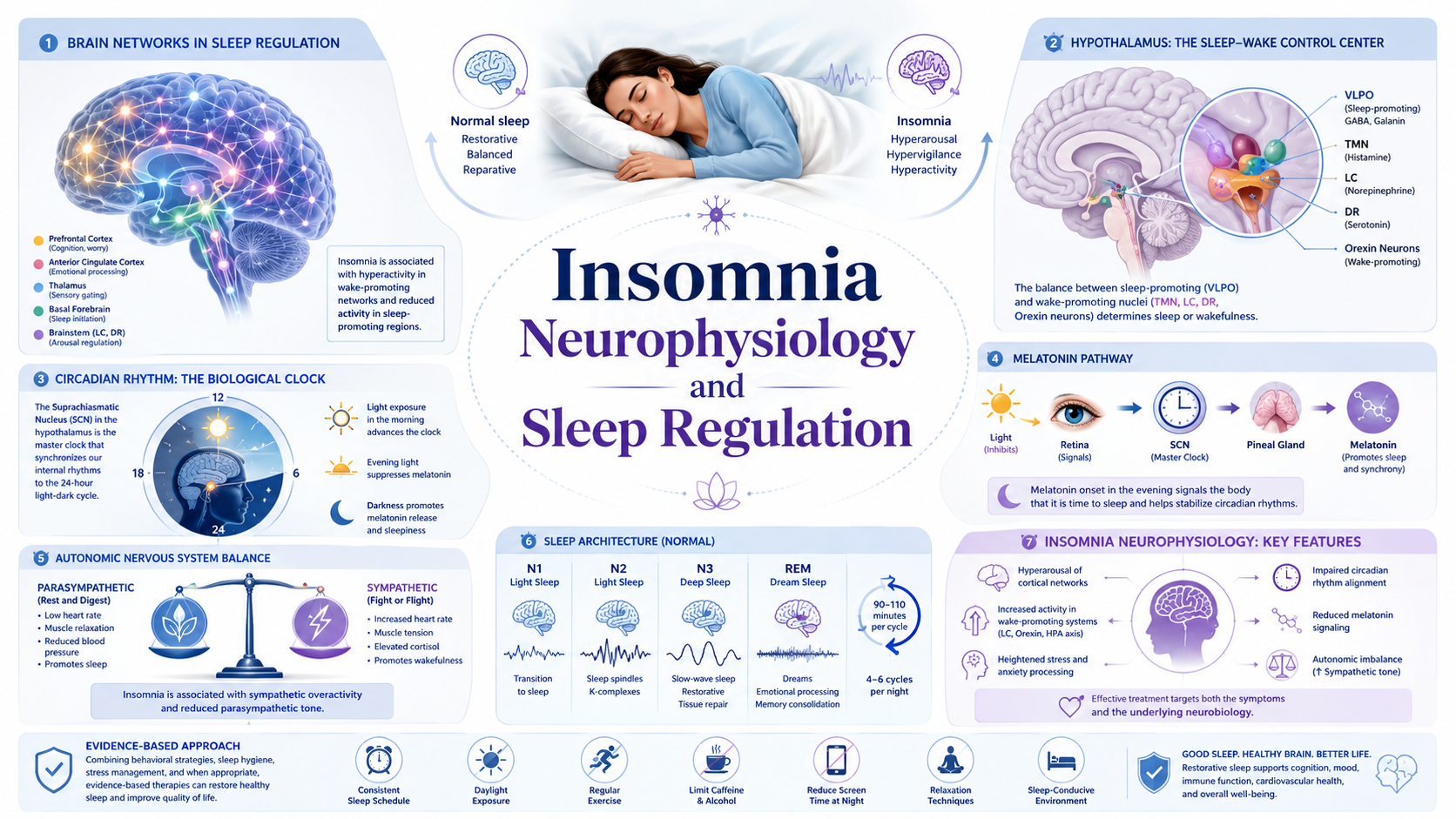
Stress Hormones and Body Responses
The hypothalamic-pituitary-adrenal axis coordinates hormonal responses to stress, including cortisol release. Repeated or prolonged stress may affect sleep, emotional regulation, working memory, and the ability to maintain attention under pressure.
Physiological responses may include muscle tension, altered breathing, fatigue, sleep irregularity, gastrointestinal discomfort, or heightened sensitivity to stimulation. These responses are not specific to ADHD, but they can increase the functional burden of ADHD executive function impairment.
From an integrated perspective, executive control is understood as dependent on both neural circuitry and the physiological state of the body. When stress regulation and autonomic balance are unstable, the prefrontal cortex may have greater difficulty maintaining reflective control over immediate responses.
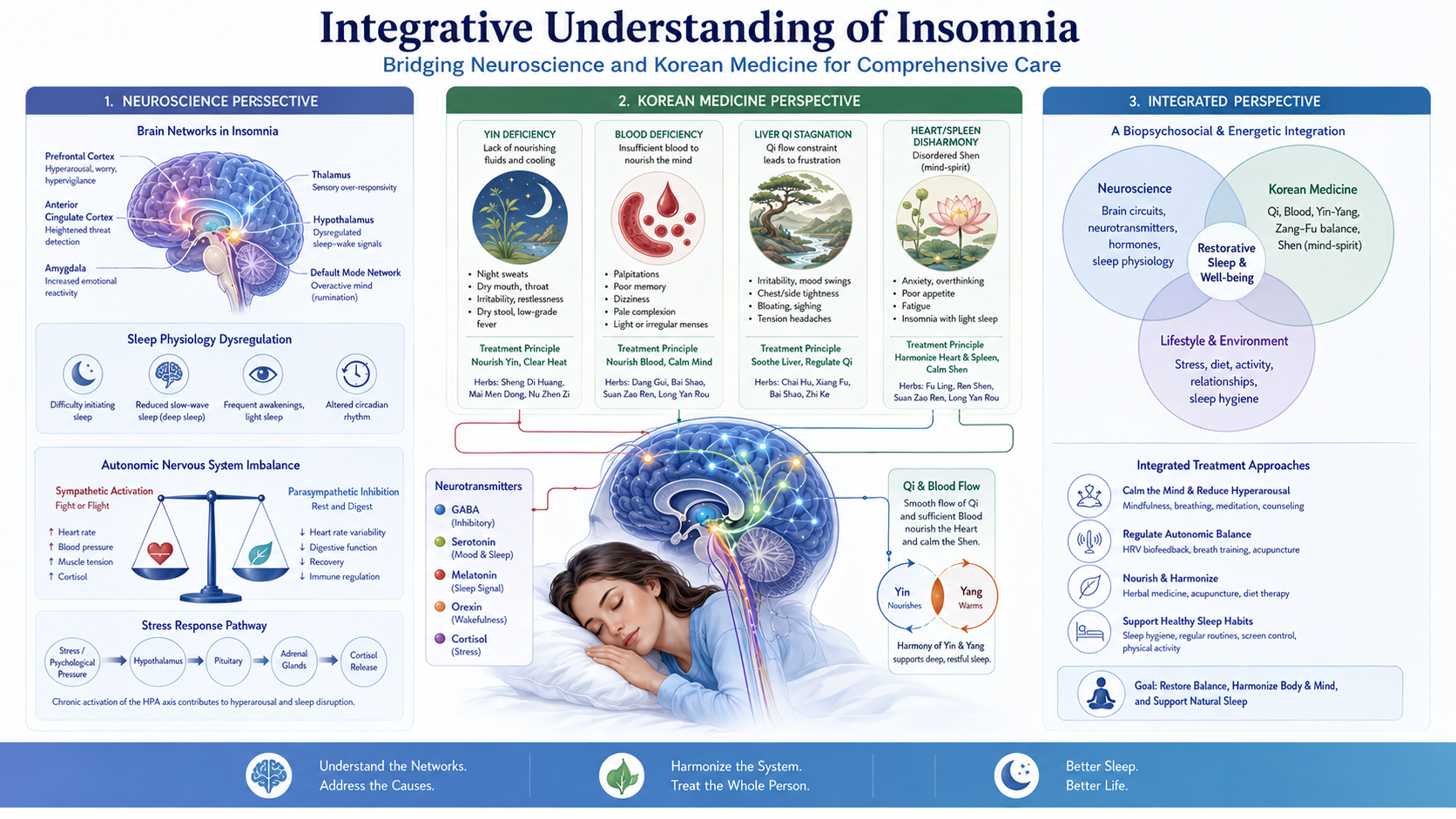
Korean Medicine Pathophysiology
Korean medicine describes ADHD-related symptoms through functional patterns rather than through one fixed disease mechanism. Pattern identification examines the relationship among attention, activity, emotion, sleep, digestion, fatigue, and constitutional tendencies. These concepts provide an explanatory framework that can be discussed alongside neuroscience without treating either framework as merely secondary.
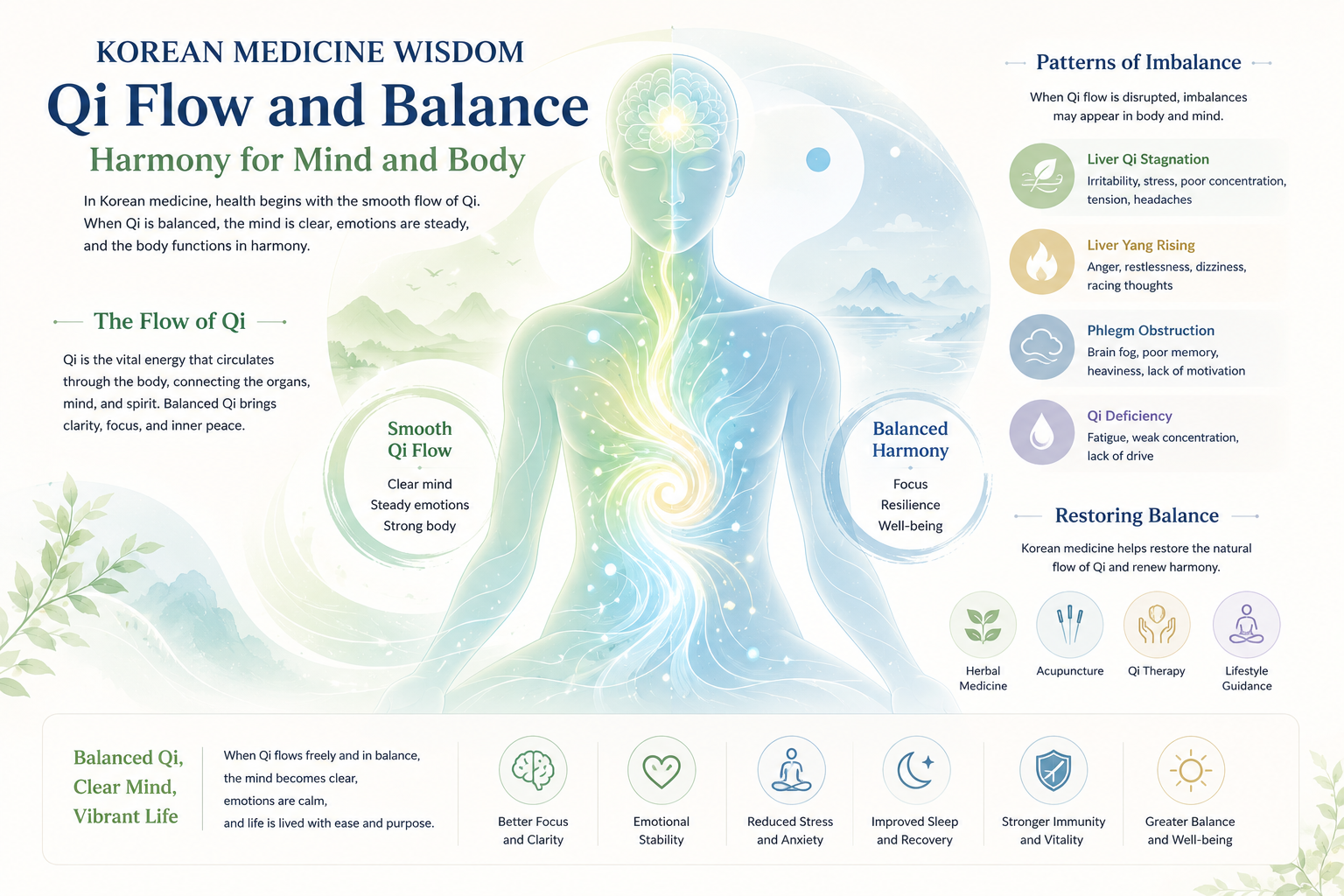
Qi and Blood Deficiency
Qi and blood deficiency is described as insufficient functional support and nourishment for sustained mental activity. It may be linked to fatigue, weak concentration, forgetfulness, inconsistent task persistence, and reduced recovery after cognitive effort.
Yin Deficiency
Yin deficiency is understood as insufficient stabilizing and restorative capacity. It may be associated with internal restlessness, sleep disturbance, irritability, and difficulty settling attention after stimulation.
Phlegm Accumulation
Phlegm accumulation is described as an obstruction of clear mental processing. It may be linked to cognitive clouding, distractibility, heaviness, delayed task initiation, and difficulty organizing thoughts.
Liver Qi Stagnation
Liver qi stagnation is associated with constrained adaptation to stress and emotional pressure. It may be linked to irritability, frustration, variable concentration, impulsive reactions, and tension-related symptoms.
These Korean medicine concepts may be functionally connected with nervous system regulation. Qi and blood deficiency may be discussed alongside reduced cognitive endurance, yin deficiency alongside impaired recovery and arousal regulation, phlegm accumulation alongside reduced mental clarity, and liver qi stagnation alongside stress-related autonomic activation.
ADHD executive function impairment is therefore understood within Korean medicine as involving both insufficient support for stable cognition and difficulty regulating activation. This interpretation corresponds conceptually with neuroscience findings concerning prefrontal efficiency, fronto-striatal communication, autonomic balance, and stress-related changes in cognitive performance.
Treatment Perspective
From the perspective of Korean Medicine Neuropsychiatry, treatment is understood as a process of supporting nervous system regulation, improving autonomic balance, and strengthening the recovery processes required for sustained cognitive control.
The treatment perspective begins with an individualized assessment of symptom pattern, developmental history, sleep, emotional regulation, stress exposure, physical condition, and functional impairment. Because ADHD is a neurodevelopmental condition, treatment is not understood as correcting a personality flaw. It is directed toward reducing impairment and improving the consistency of self-regulation.
Neuroscience-based approaches may focus on strengthening environmental structure, supporting prefrontal control, regulating dopamine and norepinephrine function, and reducing demands that unnecessarily overload working memory. Behavioral strategies may include task segmentation, external reminders, visual schedules, reduced distractions, and immediate feedback.
Korean medicine pattern-based treatment is understood as addressing the functional imbalances associated with the individual presentation. Qi and blood deficiency may direct attention toward cognitive endurance and fatigue. Yin deficiency may direct attention toward restlessness, sleep, and recovery. Phlegm accumulation may direct attention toward mental clouding and slowed task initiation. Liver qi stagnation may direct attention toward stress reactivity and emotional constraint.
The recovery process is considered to be multidimensional. Improvement may involve more stable sleep, better recognition of attention limits, reduced physiological overactivation, increased ability to pause before responding, and greater consistency in initiating and completing tasks. Changes in ADHD executive function are often more meaningful when evaluated through daily functioning rather than through concentration alone.

Summary
ADHD is described as a neurodevelopmental condition involving persistent difficulties with attention, activity regulation, and impulse control. ADHD executive function impairment is associated with inconsistent working memory, planning, inhibition, emotional regulation, and goal-directed behavior.
Neural mechanisms involve the prefrontal cortex, basal ganglia, striatum, and fronto-striatal circuits. Dopamine and norepinephrine contribute to attention, motivation, reward processing, alertness, and the maintenance of task-relevant information.
Korean medicine explains the condition through patterns such as qi and blood deficiency, yin deficiency, phlegm accumulation, and liver qi stagnation. These patterns may be linked to cognitive fatigue, restlessness, reduced mental clarity, stress reactivity, and unstable physiological regulation.
These integrated mechanisms explain how ADHD executive function affects both brain regulation and systemic balance.
An integrated perspective does not reduce ADHD to either one brain area or one systemic pattern. It explains ADHD executive function as the result of interactions among neural development, neurotransmitter regulation, autonomic state, stress response, sleep, environmental demands, and individual functional characteristics.
Korean Medicine Neuropsychiatry investigates these relationships as an active academic framework, while the Korean Society of Oriental Neuropsychiatry studies and integrates neuroscience, clinical psychiatry, and Korean medicine concepts to explain attention and behavioral regulation through complementary medical perspectives.
The keyword is included in the introduction, section text, image alt descriptions, and summary without excessive repetition.